ATLAS CORRECTION (C1)
Please scroll to the bottom of the page to enable translation for the entire text. | |
Then click the printer symbol to print the instructions in your chosen language. | |
Please note this is an automatic translation, which means there may be some errors. |

Copyright © Alastair McLoughlin 2015 Revised © Alastair McLoughlin 2019 and 2022
The right of Alastair McLoughlin to be identified as the original Designer, Developer and Author of the Work has been asserted by him in accordance with the Copyright, Design and Patents Act 1998.
All rights reserved. No part of this text may be reproduced, stored in a retrieval system, or transmitted in any form or by any means without the prior written permission of the publisher, nor be otherwise circulated in any form of binding or cover, or reprinted in any physical or electronic manner without the written consent of the author.
The ideas and concepts explored within this text are those of the author. For educational purposes only.
No diagnosis is being offered nor any cure promised by the application of this information.
Alastair McLoughlin cannot be held responsible for any injury arising from the application of this work by the practitioner to any third party however caused.
This work is not a substitute for medical attention. Please seek your physician’s advice if in doubt.
Misalignment of the AO-joint (Atlanto-Occipital joint - C0/C1) or the AA-joint (Atlanto-Axial joint - C1/C2) are more common than you may realise.
In any group of people, you may typically have between 50% to 75% positive tests for AO misalignment - or even more.
Some texts state that everyone born via the birth canal (as opposed to C-section) will probably have an AO problem - which is the reason many chiropractors routinely check and treat babies for this effect.
That all adds up to a lot of people!
There are quite a few different methods of AO/AA correction.
These tend to be complex, lengthy or expensive treatment options to achieve a positive outcome.
 INDICATIONS FOR USE
INDICATIONS FOR USEIndications are varied and many but include:
- Headaches and migraines
- Jaw pain
- Radiating pain up to the top or back of the head
- Neck pain and stiffness
- Eye problems, visual disturbances, light sensitivity
- Ear and auditory disturbances such as tinnitus, reduced hearing or hearing loss
- Shoulder pain and stiffness
- Nausea
- Fatigue
- Dizziness and balance problems including vertigo
- Upper back / thoracic pain
- Lower back or spinal and pelvic problems
Causes include:
- Birthing problems
- Blows to the head
- Whiplash injuries
- Poor posture
- Sleeping habits
- Other trauma such as falling
- TMJ misalignments
 CAUTIONS OR CONTRAINDICATIONS
CAUTIONS OR CONTRAINDICATIONS Exclude the possibility of any bony fracture due to a recent head injury by referring your client for scans or X-ray.
Refer for medical diagnosis if you are unsure about any undiagnosed medical condition.
Be aware that the biomechanics of the body can change significantly with this work.
For safety, always have your client seated on a chair with their back supported - NOT sat on a treatment table.
 Position of the patient:
Position of the patient:For assessment:
The client can be standing or seated.
For treatment:
The client should be seated on a chair with a back support in case of temporary disorientation or dizziness.
 Assessment:
Assessment:This is a two-part assessment, and a positive test (particularly of part 2) means that the correction of C1 is indicated.
Test 1: With the client standing or seated the practitioner should place the edges of both thumbs under the base of the occiput (on the occipital condyles) and check for alignment of the thumbs.
In some instances, you will not see any misalignment with this test. This is due to the occiput remaining in a ‘neutral’ position
– see video section marked with:

However, incorrect alignment will look like this
– see video section marked with:

Test 2: Stand at the left side of the client.
Palpate the tissue tension around the transverse processes of C1 vertebrae.
The exact location is about 1 centimetre inferior and 1 centimetre posterior of the mastoid process and origin of the sternocleidomastoid tendon, behind the ear.
(This is located inferiorly and posteriorly of the mastoid process as shown.)
Gently palpate tissue tension of those points
(Use your right hand to do this - usually the thumb for the left side of the neck and middle finger across on the right side of the neck.)
If you have small hands and a large client with a wide neck, then you may have to use two hands to test these points.
What am I checking for? You are feeling for a slight increase in tissue tension which is more apparent on one side than the other.
Sometimes you will feel a slight but obvious underlaying protrusion on one side.
Whether it is an increase of tissue tension, or a protrusion is felt, then this becomes the affected side.
 Application of the AoB procedure:
Application of the AoB procedure:Stand on the affected side and support the weight of the client’s head with your free hand.
If the affected side is on the left, then stand on the left side of the client and support the client’s head with your left hand.
Reverse the following instructions if the affected side is on the right.
Whilst supporting the client’s head, and with the neck relaxed and the head in a neutral position, gently ‘nudge’ the area of tissue tension with your thumb.
Force applied should be around 6 or 7 out of 10.
It is just a little firmer than a medium pressure, but as with all AoB work, no great force is involved.
 Pause:
Pause:Let the client sit for a minute or two (or longer) for sensations and reactions to be felt and assimilated.
Pause and check the client experiences no dizziness or light-headedness.
If they are dizzy or light-headed then wait for a minute or two to allow that feeling to clear itself.
Reactions may be felt inside their head, eyes, ears or through the neck, head, and shoulder areas - or even further throughout the upper and lower back, depending on how the misalignment has affected other body areas.
 Reassessment:
Reassessment:After reactions have subsided you may recheck for changes by using your thumbs at the base of the occiput (Test 1) or at the points inferior and posterior to the mastoid process (Test 2).
If the work has been applied correctly there should be changes at the occipital ridge and the tissue tension around the area of the transverse processes of the atlas should now be relaxed.
 Information:
Information: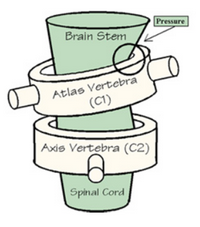 | From this image it is quite evident that any misaligment of the Atlas can cause undue pressure on the spinal cord as it emerges from the cranial cavity (foramen maagnum) impinging upon the free movement of the cerebrospinal fluid as it flows through the spine and back. | |
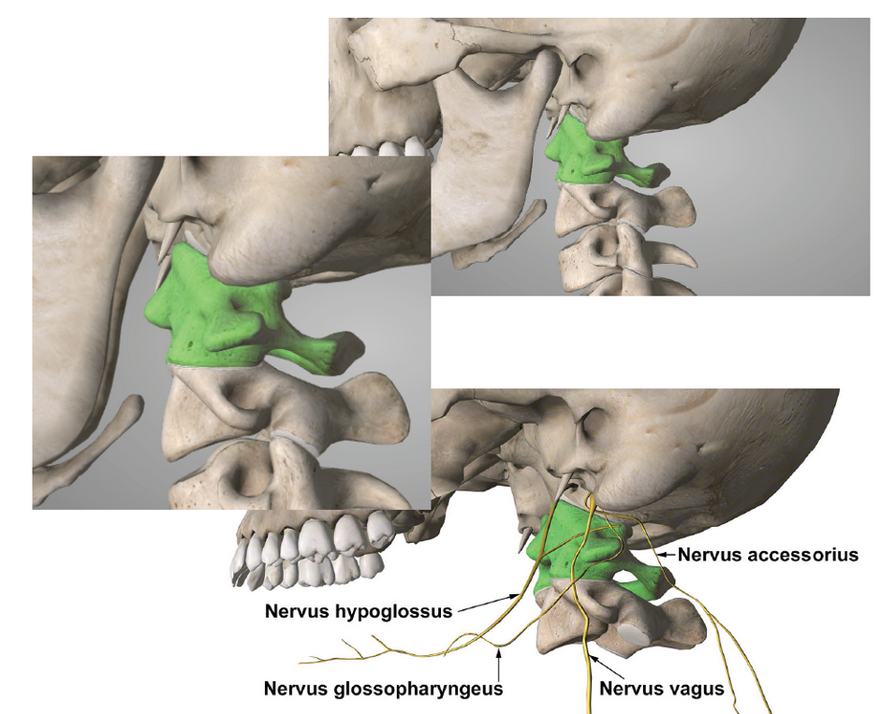 | ||
| It is worth nothing that due to the proximity of the transverse processes of the Atlas cranial nerves including the Glossopharyngeal (IX), Vagus (X), Accessory (XI) and Hypoglossus (XII) may be unduly affected. | ||